Brief overview: What is ICSI and how does it work?
In ICSI, a single sperm is injected into the inside of an egg (cytoplasm) for fertilization. ICSI treatment can address severe fertility disorders, especially in men, because sperm cells are virtually “carried to chase” during ICSI, making it possible to achieve successful fertilization of the egg even in the presence of abnormally shaped sperm (teratozoospermia), too few immobilized sperm (asthenozoospermia) or too few sperm (oligozoospermia).
Except for this procedure of fertilization of the egg in the laboratory, ICSI treatment is basically no different from IVF treatment:
ICSI usually takes several weeks. To obtain enough eggs for fertilization, the woman’s egg production is stimulated with hormones at the beginning of the treatment.
After hormone treatment, eggs are removed from the woman’s ovary. Individual sperm cells from the partner are selected and one sperm cell is injected with a very fine needle directly into each of the woman’s eggs, where fertilization is to occur.
If fertilization is successful, the fertilized eggs (= zygotes) then mature into embryos in an incubator.
Normally, up to 2 embryos are transferred into the woman’s uterus on the 2nd day after fertilization (4-cell stage) or on the 5th day after fertilization (blastocyst stage). Surplus fertilized eggs or embryos can be frozen in liquid nitrogen for later use (cryopreservation).
When should patients consider consider ICSI?
ICSI is used in various cases, especially when the causes of the unfulfilled desire for a child are to be found in the man (and possibly also in the woman):
Cause of unfulfilled desire to have children in men: in principle, only one fertilizable sperm cell from the man is required for successful ICSI. Common reasons for unwanted childbearing in men where this is the case are the following:
- The man has severed or obstructed vas deferens (obstructive azoospermia): in these cases, sperm cells can often be surgically extracted directly from the epididymis (MESA = microsurgical epididymal sperm aspiration) or the testis (TESE = testicular sperm extraction)
- The formation of spermatozoa in the testis is disturbed (non-obstructive azoospermia): in these cases, fertilizable spermatozoa can sometimes also be obtained by TESE treatment
- The man has sperm antibodies in his seminal fluid that make conception impossible naturally
- Only frozen sperm from the male are available (e.g. after certain cancer treatments such as testicular cancer)
In some cases, ICSI treatment is also used when other methods of artificial insemination have already failed, when no specific reasons for the unfulfilled desire for a child can be identified (idiopathic infertility), or when both partners have a fertility disorder.
How does ICSI work?
ICSI treatment is largely the same as IVF treatment except for the fertilization of the egg in the laboratory.
Hormonal stimulation of the ovaries (identical to IVF).
First, hormone preparations prevent the woman’s natural ovulation.
Depending on the protocol, egg stimulation begins up to 14 days later. The goal of stimulation is to have multiple follicles mature at the same time in order to obtain multiple eggs for successful artificial insemination.
Depending on the individual situation of the woman, different hormone preparations are used for hormone treatment, which are injected or also taken as tablets. The hormone FSH (follicle stimulating hormone) is often injected, which can either be injected by the woman herself or by another person.
Hormonal stimulation of the ovaries should be closely monitored by a physician, as overstimulation of the ovaries may occur in rare cases.
In some cases, hormonal stimulation of the ovaries is not used and the woman’s natural menstrual cycle is used to retrieve the eggs.
Triggering ovulation and egg retrieval (identical to IVF).
Approximately one week after starting hormone treatment, a doctor will perform an ultrasound examination to check the size and maturity of the developing eggs. In addition, certain hormone levels in the blood are measured. If the eggs have matured successfully, the hormone treatment is now stopped. Ovulation is then induced by injecting certain hormones or drugs (e.g. human chorionic gonadotropin or GnRH agonists) approximately 9-11 days after the start of hormone treatment.
36 hours after ovulation is induced, the so-called follicular puncture is performed. In this procedure, the doctor removes oocytes from the matured follicles with the help of a fine needle. Usually this procedure is performed under light anesthesia through the vagina.
In rarer cases and depending on the individual situation of the woman, the eggs are retrieved by laparoscopy – a surgical procedure through the abdominal wall that is usually performed under general anesthesia.
Fertilization of the oocytes in the laboratory and cultivation
On the day of the egg collection, the fertilization of the eggs takes place in the laboratory with the help of the ICSI method.
The sperm can either be fresh and are then often processed in the laboratory to increase their fertilization capacity and prevent allergic reactions in the woman.
Alternatively, the physician may use thawed sperm cells previously obtained by the TESE or MESA method or by other means. The thawed sperm cells must also be specially prepared.
First, hyaluronic acid is used to remove the cumulus cells surrounding the oocyte. Individual sperm cells are selected from the processed sperm cells based on appearance, shape and motility. These are then injected into one egg each under a special microscope using a very fine hollow glass needle, placed in a nutrient fluid and placed in an incubator – from this procedure comes the name of the treatment, intracytoplasmic sperm injection means that the sperm is injected into the cellular fluid (the cytoplasm) of the egg.
Within 48-72 hours, the laboratory determines whether the fertilized eggs have developed as desired for the transfer.If fertilization was successful, the fertilized eggs mature for another two to a maximum of 6 days in the incubator.
Transfer of 1-2 embryos (identical to ICSI)
Between the second and maximum sixth day after fertilization, the doctor then usually transfers 1-2 of the fertilized embryos into the woman’s uterus. This is done without anesthesia using a thin and flexible tube (catheter) through the woman’s vagina and is usually hardly painful, if at all.
Surplus fertilized eggs can be stored with cryopreservation for possible further attempt or further pregnancies.
Additional treatment: Hatching aid (Assisted Hatching)
In some cases, for example, when several unsuccessful embryo transfers have already been performed or when cryopreserved eggs are used, doctors can try to improve the implantation of the transferred embryos with a so-called hatching aid.
Usually, an embryo must implant in the uterine lining on about the fifth day after fertilization. For this, the outer shell surrounding the embryo must be thin enough for the embryo to hatch out of it. To increase the probability of success here, the outer shell of the embryo is thinned out by laser during hatching.
However, there are no clear results on the improvement of the probability of getting pregnant with this method.

Control examinations (identical to ICSI)
About 2 weeks after embryo transfer, a test of the pregnancy hormone human chorionic gonadotropin (HCG) in the woman’s blood can be used to test whether pregnancy has begun. Usually, several tests are performed to ensure a reliable result.
As with any pregnancy, an embryo or embryos can be detected by ultrasound about a month after the beginning of the pregnancy.
What are the chances and risks of ICSI?
ICSI treatment is one of the most common infertility treatments nowadays, which means that it is associated with a relatively good probability of success and relatively low risks.
Probability of success
The probability of success in an ICSI cycle to give birth to a healthy child is slightly lower than in an IVF cycle, at up to 30%. However, this is probably not because the ICSI cycle is in principle less promising than an IVF cycle, but because the cases undergoing ICSI treatment are more difficult.
Like other methods of artificial insemination, the probability of success depends on various factors, such as age, number of previous unsuccessful treatments, ovarian reserve, receptivity of the endometrium, etc.
The following graph compares probability of success of ICSI and IVF treatment across different age groups of women:

Source: German IVF Register Yearbook 2021
Fewer sperm cells needed
Compared to the IVF method, the ICSI method requires far fewer sperm cells, as in the best case a single fertilizable sperm cell is sufficient for the success of the ICSI method.
Multiple births
As with IVF treatment, ICSI treatments sometimes involve transferring two embryos instead of one to increase the likelihood of success of an ICSI cycle.
This procedure increases the likelihood of a multiple pregnancy – with the associated risk of complications (in particular, the risk of premature birth and low birth weight).
Here is an overview of the probability of live births and multiple births depending on whether one embryo or two embryos are transferred. The transfer of two embryos increases the probability of a multiple birth from less than 2% to almost 30%.
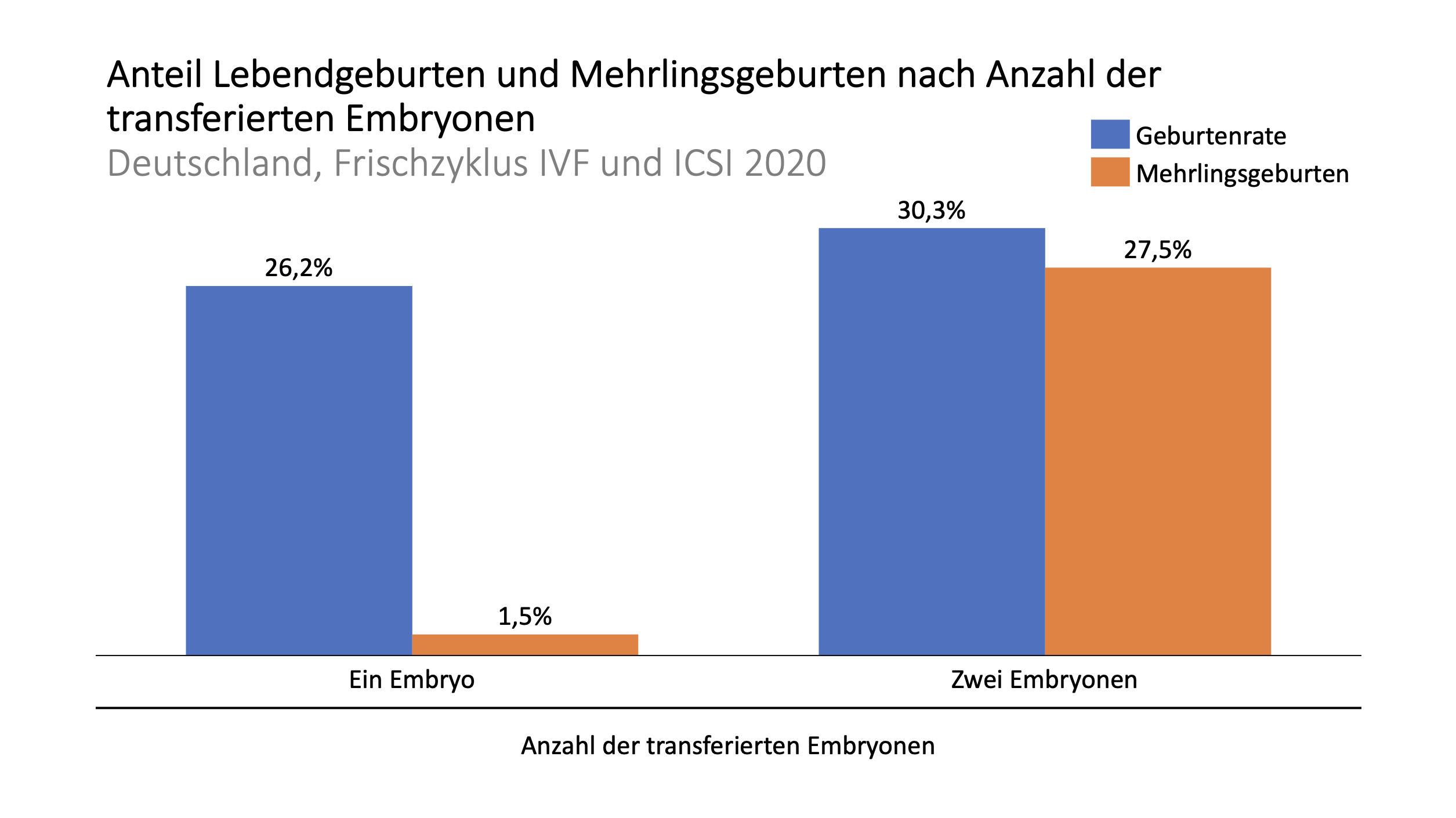
Source: German IVF Registry Yearbook 2021
Injuries and inflammations
The risk of injury and inflammation in women is identical to the risk associated with IVF treatments because the steps of treatment in women are identical.
According to data from Germany, most cases of artificial insemination proceed without complications, but there are still risks: vaginal bleeding (63% of cases) or bleeding in the abdomen (14%) may occur relatively often during egg retrieval. In addition, peritonitis (~5%) and perineal injuries in women may occur (0.2%).
Rarely, such injuries and inflammations may require hospitalization (1.3% of cases) and/or surgery in the woman (3.5% of cases).
Ovarian hyperstimulation syndrome
As with an IVF cycle, hormonal stimulation of multiple egg development can result in ovarian hyperstimulation syndrome, which causes the ovaries to swell and ache. In severe cases, this can become life-threatening.
In the past, ovarian hyperstimulation syndrome occurred in up to 10% of women undergoing artificial insemination with hormone stimulation; today, this number is less than 5%, and serious cases of ovarian hyperstimulation syndrome occur in less than 1% of women undergoing hormone therapy as part of fertility treatment.
In the case of ovarian hyperstimulation syndrome, it may be necessary, in consultation with the attending physician, to interrupt IVF treatment and temporarily freeze the embryos for later transfer to the woman’s uterus as part of a cryocycle.
Risk of TESE or MESA intervention for man
If a TESE or MESA procedure is required for sperm retrieval, it is associated with some risk of complications, as with all surgical procedures.
How much does ICSI cost?
In Switzerland, an ICSI cycle usually costs between CHF 6,000 and CHF 10,000, including the hormones to stimulate egg production. In Germany and Austria, treatment costs are somewhat lower, totaling approximately EUR 4,100 to EUR 7,300 per cycle.
In other countries of the European Union, treatment costs for IVF treatment and ICSI treatment are usually not differentiated.
The following table provides an overview of treatment costs in the DACH region and popular destinations for infertility treatment within the European Union – in line with the standard in countries outside Switzerland, Germany and Austria, IVF and ICSI treatment costs are not differentiated here. In Southern Europe (Greece and Spain) and Eastern Europe (e.g. Czech Republic), patients can save significantly on treatment costs through ICSI treatment compared to Switzerland, Germany and Austria.
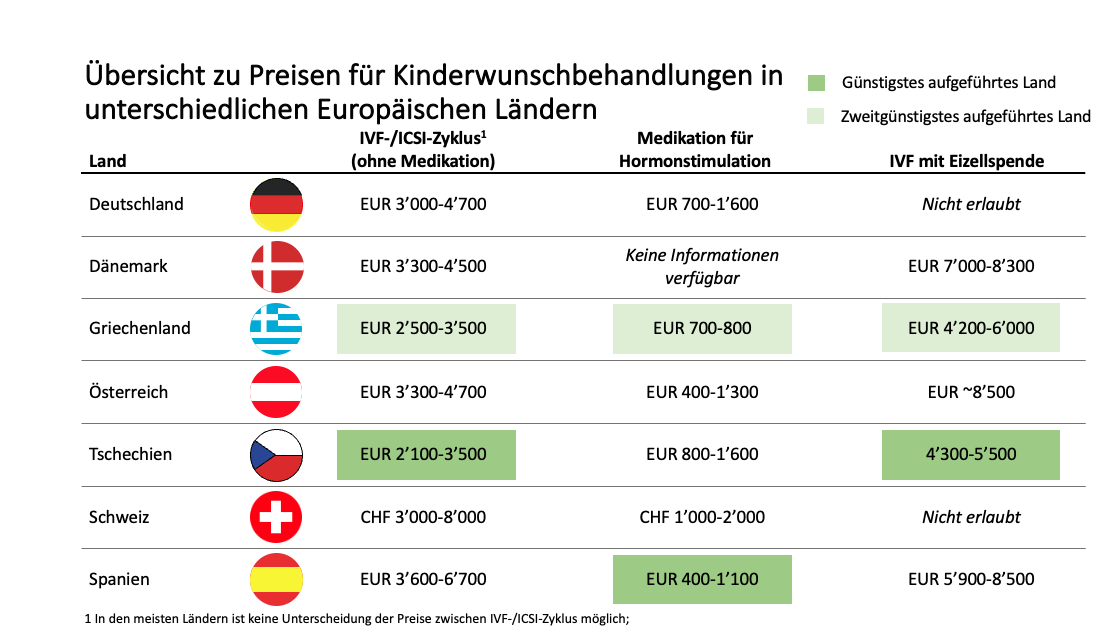
Sources: Fertilityroad.com; various fertility center price lists.
Last update: November 29, 2022
Schwierigkeiten schwanger zu werden, aber die Kosten und Mühen einer Kinderwunsch-Behandlung schrecken Sie ab?
Griechenland gehört zu den europäischen Ländern mit den günstigsten Kinderwunsch-Behandlungen. Bei Kalimedica bringen wir Sie mit Kinderwunsch-Experten zusammen und unterstützen Sie auf Ihrer Reise zur Schwangerschaft



